- More Than Teeth
- Posts
- When the Ear Is the Chief Complaint
When the Ear Is the Chief Complaint
Where Dentistry Meets Whole-Body Health Michael Bennett, DDS, PhD & Cathy Bennett, MS, NBCHWC
This is More Than Teeth. The newsletter that helps dental sleep professionals get 1% better every week.

Good Morning.
An 18-year-old patient came into my office recently with a complaint you’ve probably heard before.
"My ear feels like it’s swishing when I move my jaw."
He also had left-sided joint clicking and mild to moderate joint pain, but the ear sensation was the symptom that bothered him the most.
Here’s the twist.
He had started orthodontic treatment four months earlier, but the jaw symptoms and ear sensations existed before the braces began.
His history included playing running back on a high-school football team, multiple hard impacts, and at least two concussions. He made an observation that caught my attention immediately:
The pressure of the helmet chin strap made his jaw feel tense.
Clinically, he presented with:
• Left-side clicking on early opening
• Mild joint tenderness
• Normal range of motion
• Right-side pulsatile “swishing” sensation in the ear
My working diagnosis was:
Posteriorly displaced condyles with disc displacement, reduction, and retrodiscal inflammation.
And that’s where the case became instructive.
Key Takeaways🔑
Short on time? Here’s the clinical takeaway.
• Ear symptoms aren’t always ear problems.
Up to 40–90% of TMD patients report ear fullness, tinnitus, or pressure.
• Jaw movement changing ear sensations is a clue.
Swishing or pulsing with opening is often indicative of TMJ involvement.
• Stabilize the joint before finishing the bite.
Decompression orthotics reduce retrodiscal inflammation and joint loading.
• Airway problems often drive TMJ stress.
Sleep-disordered breathing can trigger nocturnal bruxism and joint compression.
• Treat the system, not just the teeth.
TMJ decompression, airway support, and interdisciplinary care resolve symptoms faster.
5-minute read👇
Clinical Corner
The Connection Between the Ear and TMJ That Many Dentists Miss
The temporomandibular joint (TMJ) is located right in front of the ear canal and is connected to the area around the ear through nerves and blood vessels. When the jaw joint becomes misaligned, it can affect nearby tissues, nerves, and blood vessels. This can lead to symptoms like:
- A feeling of fullness in the ear
- Ringing in the ears (tinnitus)
- Throbbing sensations
- A sense of ear congestion
- Occasional changes in hearing
Research shows that 40–90% of people with TMJ disorders also have ear-related symptoms, even if ear exams show nothing wrong. Common ear issues for those with TMJ problems include ear fullness, ringing, and pain.
The reason is simple: the TMJ and the ear share nerve connections. The TMJ is connected to the ear area by the auriculotemporal nerve, which is part of the trigeminal nerve system. Essentially, the ear and the TMJ are linked through the same nerve pathways.
The “Swishing” Ear Symptom
The patient's reported pulsatile swishing sensation is particularly interesting.
Jaw-related ear sounds are now recognized as a type of tinnitus linked to the senses, in which the jaw joint affects hearing (Levine et al., 2007). In these situations, factors such as jaw movement, pressure on the jaw joint, nearby blood vessels, and nerve changes can affect hearing. People might describe these sounds as: swishing, pulsing, fluttering, or pressure in the ear. It's important to note that these sounds may change when the jaw moves, which can help diagnose the issue.
Why Orthodontics Was Not the First Step
When I contacted the orthodontist, their response was professional but cautious.
They essentially told the family they had no opinion one way or the other.
From an orthodontic standpoint, that makes sense. Their focus is on tooth position and occlusion.
But the question airway-centered dentists must ask is different:
Can we create a stable occlusion if the joints themselves are unstable?
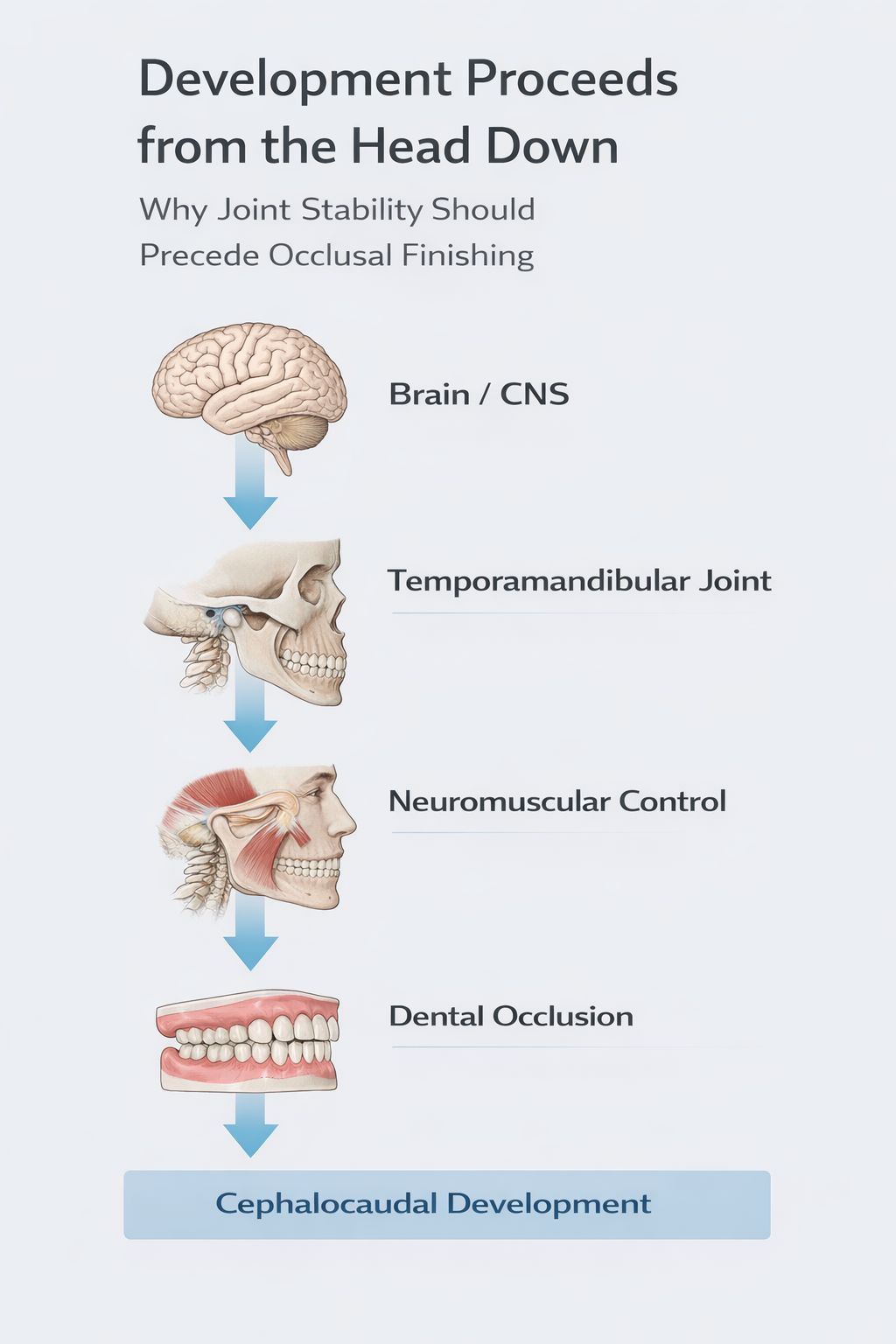
My clinical philosophy is simple:
Stable joints and airway function first. Occlusion second.
Human development follows a cephalocaudal pattern, meaning growth and neurologic control progress from the head downward. Cranial structures develop and organize before structures farther down the body (Moore et al.; Carlson; Sadler). In the craniofacial system, the temporomandibular joints sit superior to the occlusion. From a developmental standpoint, this reinforces a fundamental orthopedic principle: stable joints should guide the bite—not the other way around. Click here for references.
If condyles are compressed posteriorly and discs are displaced, orthodontic mechanics may unintentionally lock dysfunction deeper into the occlusion.
This is not a criticism of orthodontics.
It’s a question of treatment sequencing.
Phase One: Joint Decompression
For this patient, I recommended a six-month decompression phase before orthodontic finishing.
The objectives are straightforward:
Reduce retrodiscal inflammation
Allow condyles to assume a physiologic position
decrease joint loading
Stabilize the TMJ prior to orthodontic finishing
Treatment includes:
- Daytime and nighttime orthotics to relieve pressure on the jaw
- Physical therapy focused on the jaw joint
- Eating whole foods, drinking more water, and following muscle relaxation techniques
Stabilization splints can greatly reduce jaw pain and improve jaw movement by balancing joint pressure and reducing muscle tension. Occlusal appliances are also commonly used to manage issues like disc displacement and inflammation, helping the joint heal in a better position.
When the jaw joints are relieved of pressure, several symptoms often get better, such as:
- Joint pain
- Clicking sounds
- Muscle tension
- Ear symptoms
For many patients, ear symptoms improve first.
The Airway Connection
The patient was diagnosed with mild obstructive sleep apnea and upper airway resistance syndrome. His airway issues included narrow nasal passages, a crooked septum, enlarged turbinates, an underdeveloped upper jaw, a receding lower jaw, and reduced space behind the palate. These issues are common in airway-focused practices.
Sleep-breathing problems can lead to teeth grinding at night, which can put extra pressure on the jaw joints. Treatment included: improving nasal airflow, supporting nasal valves, keeping nasal passages moist (Xlear), using NightLase® laser therapy to strengthen throat tissues, and supporting the lower jaw.
Two additional referrals were suggested: seeing an ENT specialist, getting an allergy check-up. Improving airway function often reduces nighttime teeth grinding, which lessens pressure on the jaw joints.
The Trauma Component
The football history likely played a role.
Repeated impacts can contribute to:
• cervical compression
• mandibular trauma
• muscular guarding patterns
• altered condylar positioning
When trauma, airway dysfunction, and bruxism intersect, the TMJ may remain chronically overloaded.
Practical Takeaways for Airway-Focused Dentists
When patients present with ear symptoms and TMJ signs, consider three questions.
1. Could the condyle be posteriorly displaced?
Look for:
• early opening clicks
• retrodiscal tenderness
• ear symptoms without ENT findings
2. Are orthodontic mechanics occurring on unstable joints?
If symptoms are present, consider joint stabilization before occlusal finishing.
3. Is airway dysfunction contributing to joint loading?
Evaluate:
• nasal breathing
• craniofacial development
• mandibular position
• sleep symptoms
The Bigger Message
This situation shows a communication issue. Parents might get different advice from two types of dental specialists. Orthodontists mainly look at teeth and how they fit together. Airway-focused dentists focus on jaw joints, breathing, and muscle balance. Both views are valid.
However, when there are symptoms, the order of treatment is important: first, ensure stable joints, then stable teeth alignment, and finally stable airway support. Following this order usually leads to the best results.
Final Thought
Ear symptoms are one of the most overlooked clues in TMJ dysfunction.
When a patient says:
"My ear swishes when I move my jaw."
It may not be an ear problem at all.
Sometimes the ear is simply reporting that the condyle is under pressure.
And pressure is the body’s way of asking for decompression.
— Dr. Mike Bennett
Selected Peer-Reviewed References
Al-Moraissi EA, et al. (2020). Effectiveness of stabilization splints in temporomandibular disorder management: systematic review and meta-analysis. Journal of Oral Rehabilitation.
Coulter J, O’Connor S. (2024). Otalgia. StatPearls Publishing.
De Toledo IP, et al. (2017). Prevalence of otologic signs and symptoms in temporomandibular disorder patients. Journal of Oral Rehabilitation.
Edvall NK, et al. (2019). Impact of temporomandibular joint complaints on tinnitus-related distress. Scientific Reports.
Gauer RL, Semidey MJ. (2015). Diagnosis and treatment of temporomandibular disorders. American Family Physician.
Kusdra PM, et al. (2018). Relationship between otological symptoms and temporomandibular disorders. International Tinnitus Journal.
Levine RA, Nam EC, Melcher JR. (2007). Somatosensory pulsatile tinnitus syndrome. Hearing Research.
Mejersjö C, Näslund J. (2021). Ear symptoms in patients with orofacial pain and dysfunction. Journal of Oral Rehabilitation.
Okeson JP. (2014). Management of temporomandibular disorders and occlusion with occlusal appliances. Journal of Prosthetic Dentistry.
Coach Cathy’s Take
Simple Ways to Reduce Jaw Tension and Sleep Stress
When the jaw and airway are under strain at night, small daily habits can make a big difference. These simple strategies help calm the nervous system and reduce nighttime clenching.
• Prioritize nasal breathing during the day – Nasal airflow helps regulate the nervous system and reduces mouth-breathing stress on the jaw.
• Keep evening meals light and earlier – Heavy meals close to bedtime increase airway resistance and nighttime muscle tension.
• Support good sleep posture – A slightly elevated head position can reduce airway collapse and decrease jaw clenching overnight.
• Wind down the nervous system before bed – A short walk, light stretching, or slow breathing can reduce the sympathetic “fight-or-flight” tone that fuels nighttime grinding.

Until next week,
— Dr. Michael & Cathy Bennett
More Than Teeth | A Mission for Generational Health
For more podcasts and great information, check out our website here
Reply